
 |
 |
| On the left is a typical pleximeter designed after the Piorry model, which was about 2 inches long and 1 inch wide, circa 1826. | On the right is a Piorry Stethoscope incorporating ivory pleximeter (round solid ivory disk on bottom second from left) and finger thimble ivory percussor (on bottom right), circa 1828. |
 |
 |
| Burrow's stethoscope with original rubber ring around the ear piece which enabled the stethoscope to also serve as a percussion hammer, circa 1860. | An auscultation and percussion set from Russia in a leather case with a stethoscope, percussion hammer and pleximeter, circa 1870. |
 |
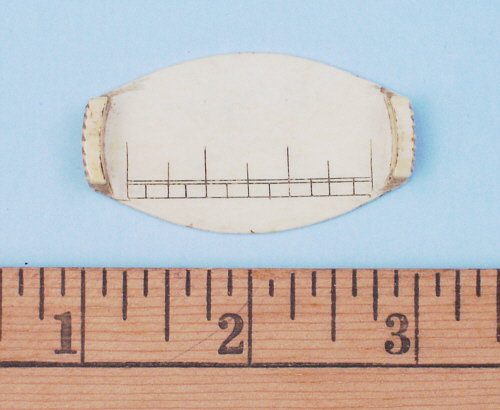
| Traube's pleximeter made of ivory, marked with a scale and with silver hinges that bend up to allow the physician to hold the pleximeter in place on the patient, circa 1850. |
 |

|
| On the left is Curschman's Percussor with Ivorine | On the right is Seitz's Percussor with ebony handle. |

|
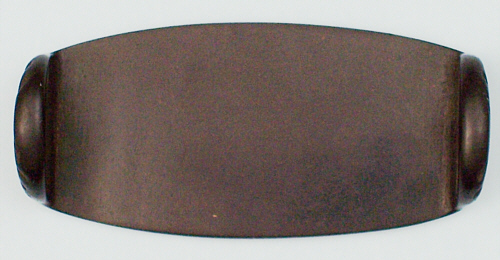
| Sibson's percussor-pleximeter, circa 1860. |
 |
 |
|
Flint's Pleximeter made of hard rubber on the left and Flint's Percussor with rubber head and hard rubber handle on the right, circa 1880. |
|